A system failing those it was built to serve April 2026
Foreword
Dr Tim Nelson
Founder and CEO at Front Foot Health
As both a clinician and a veteran, I approach this system from two perspectives: as a provider of care, and as someone who has relied on it.
This report reflects a growing tension between clinical best practice and system design.
Modern healthcare is built on principles of patient-centred care, continuity, and accessibility. These are not aspirational concepts — they are fundamental requirements for effective treatment, particularly in populations with complex and chronic conditions such as veterans.
The findings presented within this report suggest that, in several key areas, current policy settings are diverging from these principles.
Importantly, this report does not argue against reform. In fact, we are pushing for it. Veteran health systems must evolve.
However, the effectiveness of reform depends on how it is implemented — particularly the extent to which it incorporates the perspectives of those it affects.
The current approach to veteran healthcare and reform, led by the Department of Veterans Affairs, does not involve meaningful consultation with the veteran cohort or their treating practitioners.
Kneejerk policy changes, driven solely by budget considerations, are a sure way to even further restrict access to critical treatment for one of our most medically complex cohorts.
From a clinical standpoint, the themes emerging in this report — access barriers, administrative burden, constraints on treatment pathways, and lack of trust — warrant careful but immediate consideration. These factors have direct implications for patient outcomes.
This report provides a valuable evidence base to inform that discussion. It is our hope that this report will act as the voice of Australia’s veterans, as they speak out for more choice, better access, improved health supports, and a patient-driven system which not only understands their needs but prioritises them.
Executive Summary
A national survey of 1,141 Australian veterans was conducted in February 2026 and reveals a system under pressure and a veteran community that is increasingly losing confidence in it.
Key findings include:
- Trust in DVA sits at just 2.6 out of 10, with nearly 80% rating it 3 or lower
- 89% of veterans say they are not meaningfully consulted before major policy changes
- 94% believe they should choose their own healthcare providers 65% say they do not have genuine choice in how services are delivered
- Mental health is critically low, averaging 2.8 out of 10 42% say removing telehealth would disrupt their access to care
Taken together, these findings point to more than dissatisfaction.
They point to a system that veterans increasingly feel is being done to them, not with them.
What veterans are telling us
Mental health is at a critical low
Veterans report an average mental health rating of 2.8 out of 10.
At the same time, more than 40% say they cannot reliably access mental health support when they need it.
This is one of the most confronting findings in the report.
Low mental health scores at this level indicate a population experiencing significant psychological and psychiatric strain. When combined with inconsistent access to care, it raises serious questions about system responsiveness to one of the most critical areas of veteran health.
Given our country has conducted multiple parliamentary inquiries and investigations into how to lower veteran suicide rates, this finding should shock our entire government into immediate action.

A collapse in trust
Trust is the foundation of any healthcare system. Without it, even well designed services struggle to function effectively.
Right now, that foundation is weak.
Nearly four in five veterans rate their trust in DVA at 3 out of 10 or lower.
This reflects a sustained erosion of confidence in the institution responsible for delivering veteran care.
When trust falls to this level, it begins to influence behaviour — including whether veterans seek care, adhere to treatment or engage with the system at all.
4 in 5 veterans don't trust DVA

Rating it 3/10 or lower
Decisions made without them
Almost 9 in 10 veterans say they are not meaningfully consulted before major policy changes.
This points to a structural absence of stakeholder engagement in decision making processes.
Decisions affecting treatment pathways, access and eligibility are being made without the consistent input of those directly impacted.
Over time, this creates a disconnect between policy intent and lived experience and it is often in that gap where trust deteriorates most rapidly.
9 out of 10 not meaningfully consulted

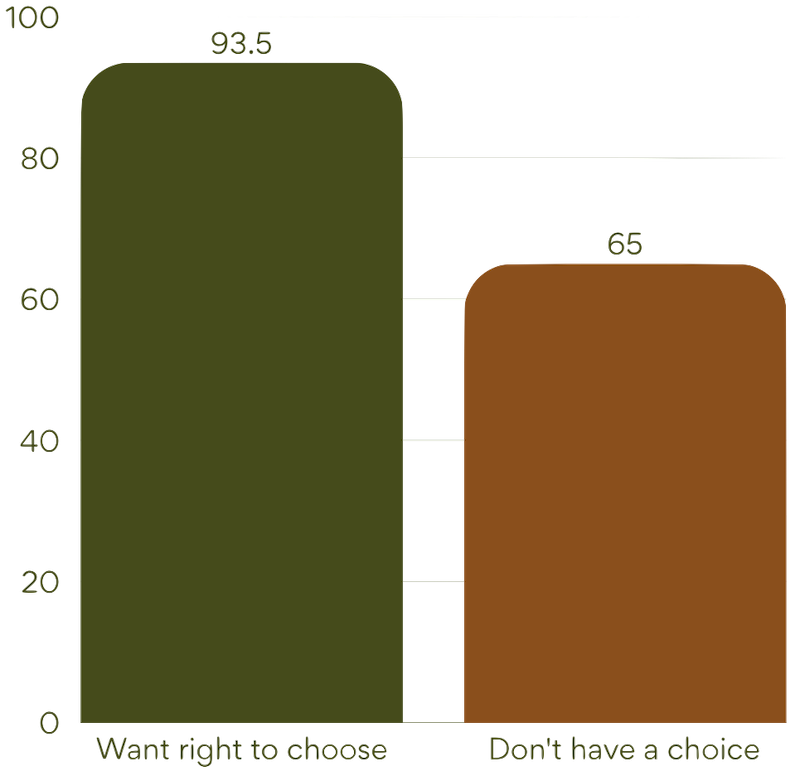
Choice is being eroded
The message here is unequivocal:
- 93.5% want the right to choose their provider
- Yet 65% say they do not have genuine choice in practice
This gap between expectation and experience for our veteran cohort is significant.
Choice in healthcare is not simply about preference — it underpins continuity of care, therapeutic relationships and, most importantly, patient confidence. When veterans feel that choice is being constrained, it can lead to disengagement and fragmented care.
Changes brought in by the Department in February 2026 further reduce choice for veterans, and instead push them into a single provider model via the government’s tendered provider.
This not only removes veteran autonomy, but it further increases the lack of trust veterans have in the system.
The relationship between a veteran and their treating GP should be of utmost importance to the Department and the government, but current changes show it is not.
Access is getting harder
Nearly one in three veterans report delays accessing treatment, while many identify administrative burden and policy restrictions as key barriers.
This points to systemic friction within the way care is accessed and delivered by Australian veterans.
For a population with complex, often chronic conditions, delays and administrative complexity are more than inconveniences. They can often disrupt treatment continuity, exacerbate health conditions, increase reliance on acute care pathways, or result in the patient not seeking support at all.
Over time, these barriers accumulate and create a system that feels increasingly difficult to navigate and it often pushes veterans out completely, where many self-medicate or don’t receive treatment at all.
1 in 3 veterans delayed accessing treatment
What this means
Individually, each of these findings is concerning.
Together, they point to something more significant: a system experiencing cumulative pressure across trust, access and responsiveness.
This is not about a single policy decision or isolated failure. It is about a pattern:
- Decisions made without consultation
- Restrictions introduced without clear alignment to patient need
- Structural barriers that build over time rather than being resolved
The risk is not only declining satisfaction. It is gradual disengagement from the system itself.
And increasingly, that is what veterans are saying.
Recommendations
To rectify this concerning situation, the below recommendations should be implemented as a matter of government urgency.
-
Enshrine veteran choice of treating practitioner as a non negotiable principle across all DVA-funded care.
-
Establish a clear, consistent, and legislated definition of “treating practitioner” to prevent arbitrary exclusion.
-
Remove structural barriers that direct veterans toward DVA appointed providers over their chosen clinicians.
-
Ensure telehealth access is available on equal terms for all providers, not limited to government-contracted services.
-
Align fee schedules with true cost of service and ensure parity between DVA-appointed providers and independent clinicians.
-
Fund and reduce administrative burden on clinicians to prevent provider withdrawal from veteran care.
-
Guarantee access to clinically appropriate diagnostic investigations regardless of provider type.
-
Eliminate bottlenecks by allowing veterans to access assessments through their own practitioners rather than a single contracted provider.
-
Prohibit the overriding of clinical judgement by administrative processes, particularly in determining condition stability and treatment pathways.










.png)





